A Primer in Immunotherapy – A Simple Guide for Everyone
INTRODUCTION
I was recently invited to be part of a panel in a Channel News Asia (CNA) programme called “Perspectives”, which is a live audience recording to discuss the role of immunotherapy in treating advanced lung cancer.
A type of immunotherapy called pembrolizumab was recently approved by the US Food Drug Administration (FDA) for use in first-line therapy for a subtype of lung cancer that is highly responsive to such agents. As I am preparing for the CNA programme, I quickly realized that it will be impossible for the panel of experts to impart even a basic understanding in that short space of time.
A primer of immunotherapy for the layperson devoid of jargon will hopefully be useful in establishing a basic understanding of how the immune system works against cancer growth and how we may exploit this knowledge in the development of immunotherapy.
We Are Stronger Than We Think – How Our Immunity Prevents Normal Cells Turning Rogue
Every few seconds, a cell turns rogue in our body and there is a definite potential for it to become cancerous. The causes for it turning rogue are varied – it may be environment related carcinogens, radiation, viral infections, chronic inflammation or inherited genetic mutations.
It is as if a computer virus has entered the cell software programme instructing the cell to behave in a bizarre uncontrolled manner. Our well-tuned immune system shuts down the rogue cell and disintegrates it before matters get out of control.
Who are the players in our immune system doing this important policing job?
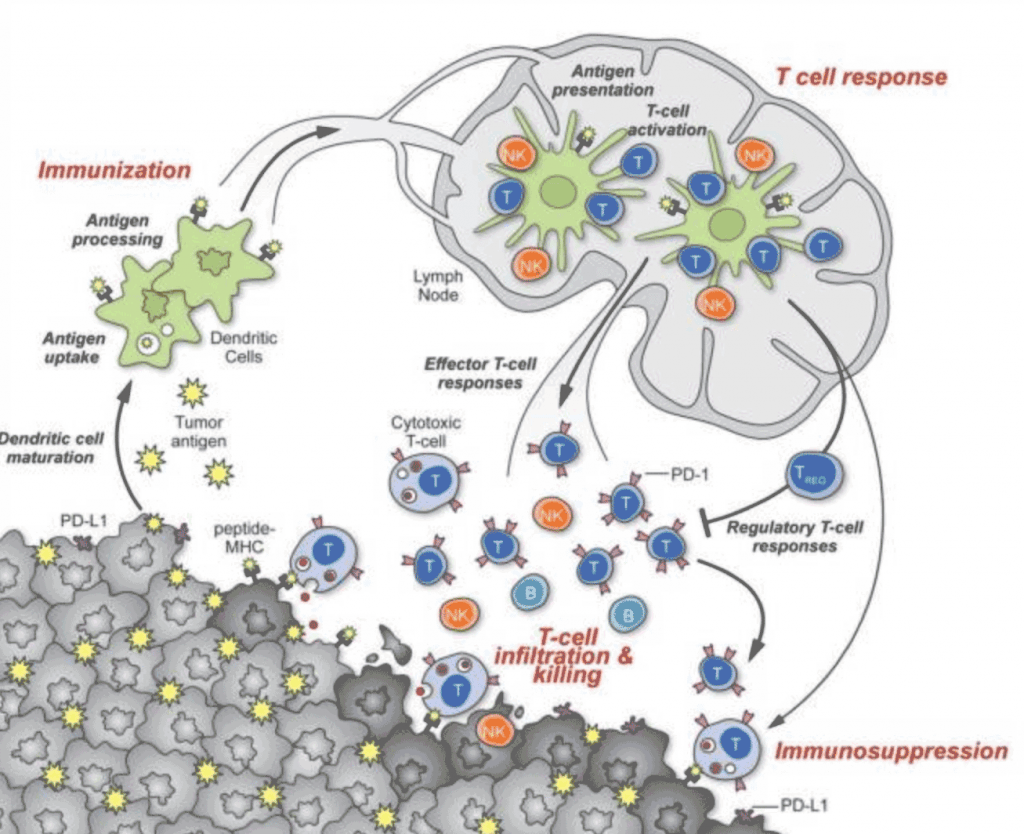
- The T-cells – there are 2 types, the cytotoxic T-cells (T-C) and the helper T-cells (T-H). They are crucial in allowing the body to recognize the rogue cells from the normal cells. They need the assistance of the matchmakers to bring the rogue cells to them for recognition and activation. These matchmakers are known in science as antigen presenting cells (APCs).
Cytotoxic T-Cells (T-C), Helper T-cells (T-H), Antigen Presenting Cells (APC)
- Natural born killer cells – these are the Sherman tanks in the assault division of the immune system that punches a huge hole in the enemy. These aggressive killer cells are not shy and need no matchmaking introduction at all by APCs.

Natural Born Killer Cells
- The Firefighters – a population of such cells are officially known as the T regulatory cells that put out the flames when the cytotoxic T-cells become over exuberant in flaming the rogue cells. A deficiency of these firefighters results in the immune system becoming so overwhelming that it turns upon normal body tissue and cells. A condition we call autoimmune disorder.

T regulatory cells
- The Scavengers – these cells are called macrophages and they scavenge by literally swallowing up the cancer cells whole (‘Pacman activity’) after being activated. They serve well by mopping up ailing rogue cells.

Macrophages Cells like Pacman
The above 4 main types of cells act in concert to keep the rogue cells at bay. After the coordinated action, the Firefighters come in to douse the flames of the cytotoxic T-cells before they affect normal cells too.
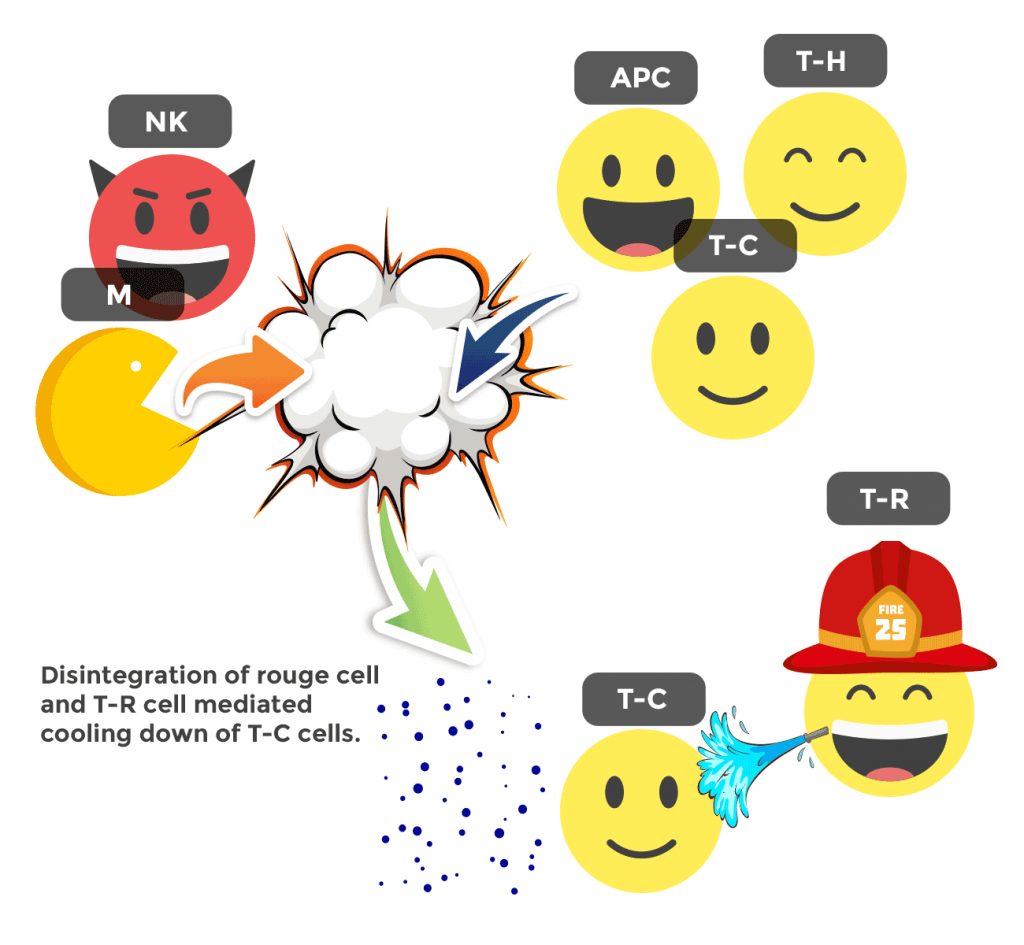
Cells working together to fight rogue cells
We were never always this clever to have devised the workings of our immune system against cancer right from the beginning. This is the part that gets interesting. We shall now walk through the corridors of history to catch a glimpse of how we strove to harness the immune system to treat cancer. Let’s look at the many ways this may be done.
Using Infections To Stimulate The Immunity Against Cancer
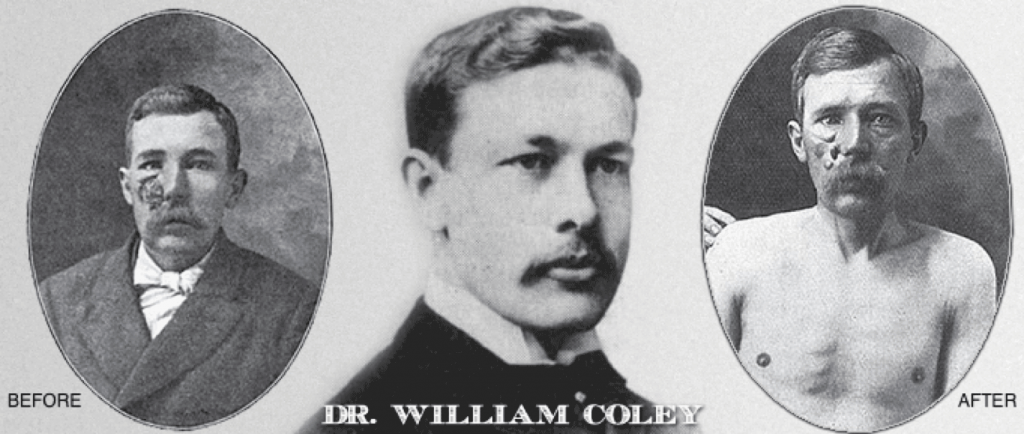
Dr William Coley – Sarcoma Treatment
1891 – A New York surgeon Dr William Coley noticed that spontaneous remissions of a soft tissue cancer called sarcoma were seen in patients after they had suffered a skin infection called erysipelas caused by a common bacteria found in the throat.
He experimented by injecting this same bacteria (Streptococcus pyrogenes) into tumours in a bid to stimulate the immune system to mount a response against the tumour in the same way with equal success. Although some tumours do recede using this method, the response is rarely durable and could not be reliably replicated in all patients. This was the first instance in modern times that infective agents have been used to stimulate the immune system against cancer.

Insertion of BCG incite an immune response in the urinary bladder
1929 – Dr Pearl from Johns Hopkins Hospital reported low cancer incidence in people who died from tuberculosis in an autopsy series and proposed that the immune system being stimulated by the tuberculosis bacteria has kept cancer cells at bay.
This led to experiments using the inactivated strain of tuberculosis called BCG (Bacille de Calmette et Guérin) to incite an immune response in the urinary bladder to treat superficial bladder cancer.
In 1976, clinical trials done showed that this method of instilling BCG into bladders whose lining were affected by cancer successfully kept recurrence at bay in the majority after surgery. BCG therapy is now a mainstay and good example of how immunotherapy is routinely employed to treat bladder cancer in mainstream medical science.
In the above 2 examples, the T-cells with APCs, Natural-born Killer Cells, Scavengers and Firefighters are all riled up in a very non-specific way.
Calling On Mr Right

Cytotoxic t-cells
Using infections to stimulate the immune system is a crude and imprecise method. Let us now turn to something more specific. We have been introduced to T-cells.
Allow me to introduce Dr Steven Rosenberg the hero of modern day immunotherapy who has for more than 40 years attempting to harness Mr T-cell to fight cancer cells.

Dr Steven Rosenberg the hero of modern day immunotherapy
1968 – Dr Steve Rosenberg was a young surgeon who was called to do a routine gallbladder removal operation in a cancer patient. Make it ex-cancer patient. This patient was diagnosed with stage 4 stomach cancer that has spread to the liver in 1956. He was not supposed to be alive!
Steve Rosenberg was intrigued. He could not find any evidence of tumours in the liver during the gallbladder operation. This man’s immune system has somehow eliminated the stomach cancer cells that metastasized to the liver. Believing that the conquering T-cells may still be lurking around in his blood, Dr Rosenberg asked for some of his blood to be transfused to another patient who was dying of stomach cancer. Unfortunately, that did not work, but it was the start of a long journey of discovery for this young surgeon.
1970s – Dr Rosenberg harvested T-cells from all sorts of sources to be infused into patients with cancers and met with little success. The main reason being the rejection of these T-cells recognized as “foreign” by the patients’ immune system. He then took on a different strategic direction by using a substance called IL-2 (Interleukin-2) hoping to stimulate the patient’s T-cells in a more specific way.
1984 – Linda Taylor a naval officer was the first patient after more than 60 patients treated by Dr Rosenberg to achieve complete remission with the use of IL-2 therapy against her condition of a rare skin cancer called melanoma.
Thirty years on, she remains well without evidence of recurrence. IL-2 went on to be approved for use by US Food Drug Administration (FDA) in melanoma and kidney cancer. However, cures experienced by patients like Linda Taylor are rare even in these cancers. There were lots more that were not well understood.

Dr Rosenberg & cancer (melanoma) survivor Linda Taylor
High dose IL-2 survived as the only FDA approved immunotherapy against melanoma and renal cell carcinoma well into the 2000s. The response rates were low (about 15%) and the side effects of an immune system unleashed against the body’s normal cells were worse than conventional chemotherapy. In fact for high dose IL-2, we had to admit the patient into ICU while using it to monitor for life-threatening side effects.
Another substance called interferon (IFN) was also used to stimulate the T-cells against cancer cells. Both IFN and IL-2 were most commonly used to treat melanoma and kidney cancer as these 2 types of cancers were then thought to be the ones which are most amenable to immunotherapy because of the relatively higher rates of spontaneous regressions in them. Again, we shall be proved wrong and we shall see why in just a while.
A variation of this method is to harvest the T-cell population and remove them outside of the patient’s body or retrieving them from the tumour tissue obtained post-surgery for culture and expansion by IL-2 and a host of other factors before reinfusing them back to the patient’s body again, hence avoiding the toxic effects of IL-2 which was used to expand the relevant T-cells outside and not inside the body.
Borrowing T-cells For A New Approach

Utilisation of T-cells to combat cancer cells
Although not considered as immunotherapy, bone marrow transplants do have an element of T-cells utilization to combat cancer cells. We have known for a long time that patients with a blood cancer called leukemia do better when they undergo bone marrow transplantation using an unrelated bone marrow match compared to a closer match among relatives. Why is this so? This is called the “graft versus leukemia” (or GVL) effect.
Although the bone marrow transplantation is primarily done to replete marrow function after ablation with high dose chemotherapy, this GVL effect is not insignificant in facilitating a better curative outcome. Although over-exuberant graft T-cells activity may also incite a “graft versus host” (GVHD) condition and turn the guns on normal body tissues.
Why will it work now when Dr Rosenberg did a similar experiment using his patient’s blood to be transfused into another as immunotherapy and failed? This is because with the high dose chemotherapy prior to the donor marrow stem cell transfusion, the recipient host environment will not mount an immune response to reject the donor T-cells.
Now they can do the job of recognizing the tumour cells better and attacking them. With greater mismatch, the antigens of the cancer cells are recognized even better as foreign and deserving of T-cell recognition and extirpation. In this setting, it is even possible to do periodic donor lymphocyte infusion (DLI) for the donor T-cell population in the patient to be kept up to continue the immune action against the cancer cells. All these are called adoptive T-cell therapy.
Increasing The Number of Roads Leading To Rome
Let us take pause and review the mechanisms that we have discussed thus far in manipulating the immune system to better fight cancer. All the following have in common is the bid to improve on the cancer-busting T-cell population quantitatively.
- Using bacterial infections to stimulate immunity in a blunderbuss manner.
- Using biological factors like IL-2 and IFN to stimulate the T-cell population inside or harvesting them to be expanded outside the body before reinfusing them.
- Using T-cells from another person.
Improving The Roads
In this next section, we shall see how the qualitative aspects of T-cell immunity against cancer may be tweaked.
Remember APCs? They are also known as dendritic cells (DCs).
They are the matchmakers. They bring the cancer cell proteins to the T-cells for the cancer cells to be recognized and for the needful response of the T-cells to happen.
This process may be harnessed as immunotherapy too leading to the development of cancer vaccines. This is similar to vaccinating our bodies against viruses. It exploits inactivated particles form the virus or bacteria through injections into our bodies to incite our immune system to be ready to ward off the real active disease causing infections when they occur.
Dendritic cells working to incite our immune system
These APC / DC matchmakers need to be primed by a protein called an adjuvant and also re-engineered outside the body to load it with a warhead – the tumour protein we call an antigen before they are presented to the T-cells to enable optimal recognition of the enemy and consequent stimulus to hunting and cell kill activity.
An example of an FDA approved cancer vaccine is Provenge® used to treat prostate cancer. Cancer vaccines are already a part of the standard treatment landscape.
Removing The Brakes
Another way to qualitatively change the way the T-cell has been interacting with the cancer cells would be to remove the T-cell evading tactics adopted by the cancer cell. This is done in mainly 2 ways for immunotherapy proven to be successful in clinical use.
Removing T-Cell in Immunotherapy
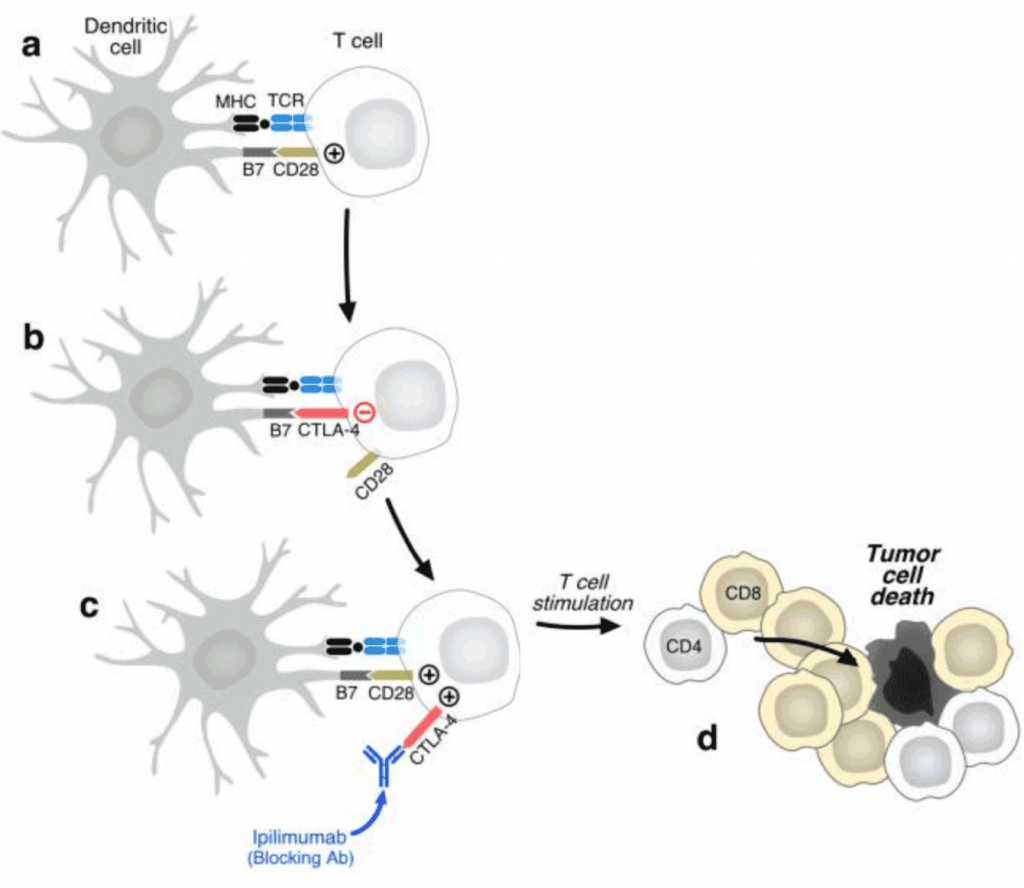
Let us zoom in on the interaction between the matchmaker and the T-cell using a microscope of the highest power and the finest resolution. Usually the T-cells after a period of being stimulated will start to express this protein called CTLA-4 which is a checkpoint protein upregulated to prevent overheating of the immune system.
When CTLA-4 starts to be expressed on the T-cell surface in greater quantities after a period of matchmaking and stimulation, they will bind to a receptor on the matchmaker known as B7 and stop the stimulation of the T-cells.
The trouble in patients with cancer is an underperforming immune system, not an overheating system. With such a logical target in CTLA-4, a drug has been designed to block CTLA-4 to allow the stimulation to continue unabated. This drug is called ipilimumab. For drugs whose names end with a “mab”, they are monoclonal antibodies against specific proteins.
Ipilimumab has been used with success in treating melanomas. But the side effects tend to be quite severe in some people treated using ipilimumab as we can see how T-cell stimulation is now unblocked and continues unrelentingly. Normal organs and body tissues get caught in the unbridled T-cell action.
Unmasking The Enemy
Next we look at another mechanism which is similar to impairing the CTLA-4 brake but subtly different in a more tumour specific way as this action takes place at the effector phase further downstream whereas CTLA-4 blockade takes place further upstream at the priming of T-cells by DC/APCs phase. This results in less immune related side effects compared with iplimumab use.

Pembrolizumab binds to the PD-1 receptor and prevents the cancer cell expressed PD-L1 from biding to PD-1 receptor and tricking the T-cell to go into deep sleep.
At last there is use for immunotherapy in a common cancer. Pembrolizumab was recently approved for use in lung cancer as first line treatment if the tumour expresses more than 50% PD-L1 protein on its surface. What is PD-L1 protein? This is a protein the cancer cell uses to evade T-cells. PD-L1 binds to the PD-1 receptor on the T-cell. PD-1 acts like CTLA-4; when it is bound by PD-L1, it sends
What is PD-L1 protein? This is a protein the cancer cell uses to evade T-cells. PD-L1 binds to the PD-1 receptor on the T-cell. PD-1 acts like CTLA-4; when it is bound by PD-L1, it sends signal to within the T-cell to disengage T-cell killing of the cancer cell. The drug pembrolizumab binds to the PD-1 receptor and prevents the cancer cell expressed PD-L1 from biding to PD-1 receptor and tricking the T-cell to go into deep sleep.
Creating X-men T-cells – CAR T (Chimeric Antigen Receptor T-cells)
The last method of design in immunotherapy involves re-engineering the proteins on the T-cells called receptors to better recognize specific proteins on the cancer cells hence logging them on better for the bull’s eye. These T-cells are harvested from the patient and their receptors re-engineered outside of the body to target the specific type of cancer cell the patient has.
The T-cells are re-engineered by way of inserting viral carried genetic code into the T-cell DNA to produce a receptor that is a mixture of the innate T-cell component and the newly coded protein scaffolding that will allow very avid latching onto the cancer cells targeted.

Car T-Cell infusion for acute lymphocytic leukemia and lymphoma containing a B-cell antigen B
CAR T is used at present to treat a certain type of leukemia we call acute lymphocytic leukemia and lymphoma containing a B-cell antigen B19. There are potential side effects including the loss of normal B cells of the immune system rendering the patient very immunosuppressed and in need of intense care.
Completing The Immunotherapy Manual
We have looked at an additional 3 steps in the qualitative improvement of immunotherapy against cancer:
- Cancer Vaccines
- Blocking the brakes in T-cell being primed for action by DCs.
- Blocking the brakes produced by cancer cells to lull T-cells into sleep
- CAR T – chimeric antigen receptor T cell
Lastly, immunotherapy may be combined with chemotherapy in unique ways to improve on cancer control outcomes. Pembrolizumab when combined with chemotherapy yielded response rates far higher compared to chemotherapy alone. Nobody really knows why and how.
About 10 years ago, I designed a combination therapy called OXAFI in a clinical trial setting to treat liver cancers, it was an intriguing journey. The very first patient with advanced liver cancer treated with OXAFI achieved a complete pathological response and she is still well and alive today. As it is not desirable to confer bias in my own blogging and writing, best not to dwell at length on my pet topics. If you wish to know more, you may check out this paper: https://core.ac.uk/download/pdf/81182679.pdf. I have also since lectured and given talks extensively on OXAFI.
It is exciting to see immunotherapy come of age after more than 100 years. There are so much more discoveries to be made and gems to be uncovered. This is only the beginning and our knowledge is the tip of the iceberg.