Translating Science Into Hope: My Takeaways from ASCO 2026
Table of Contents
- Pancreatic Cancer: New Targeted Drug in Trial
- Lung Cancer: Bispecific Antibodies Show Promise
- Sarcoma: First Targeted Treatment for a Rare Type
- Prostate Cancer: Combining Hormone Therapy With Surgery Shows Improved Outcome
- Colorectal Cancer: More Treatment Options
- Breast Cancer: Smarter Chemotherapy, Less Surgery & New Options for Advanced Cancer
- Treatment Beyond the Tumour
- What This Means for Cancer Patients and Families
Every June, the American Society of Clinical Oncology (ASCO) holds its Annual Meeting, where oncologists from around the world gather to share the results of the biggest cancer trials of the year. This year’s meeting, themed “The Science and Practice of Translation,” delivered a collection of some of the most exciting news I’ve heard in recent years for pancreatic cancer.
In this update, I’d like to share what stood out to me, and why I think patients and their families battling some of the hard-to-treat cancer types have real reason for hope.
Pancreatic Cancer: New Targeted Drug in Trial
Pancreatic cancer is one of the toughest cancers that I treat, with an overall 5-year survival rate ranging between 5–15%. Targeted therapy has long been the frontier for pancreatic cancer treatment, yet few patients were eligible. When they were, it could bring them a “new lease of life”, as reported for one of my patients in 2021, who had a rare genetic alteration in her tumour and was treated with a targeted drug called erdafitinib.
It is heartening for me listening to the results of the pivotal phase III RASolute 302 trial. The new targeted drug daraxonrasib works for the 90% of patients who carry the KRAS mutation it is designed to target, including metastatic cases. Far more patients can now benefit from it.
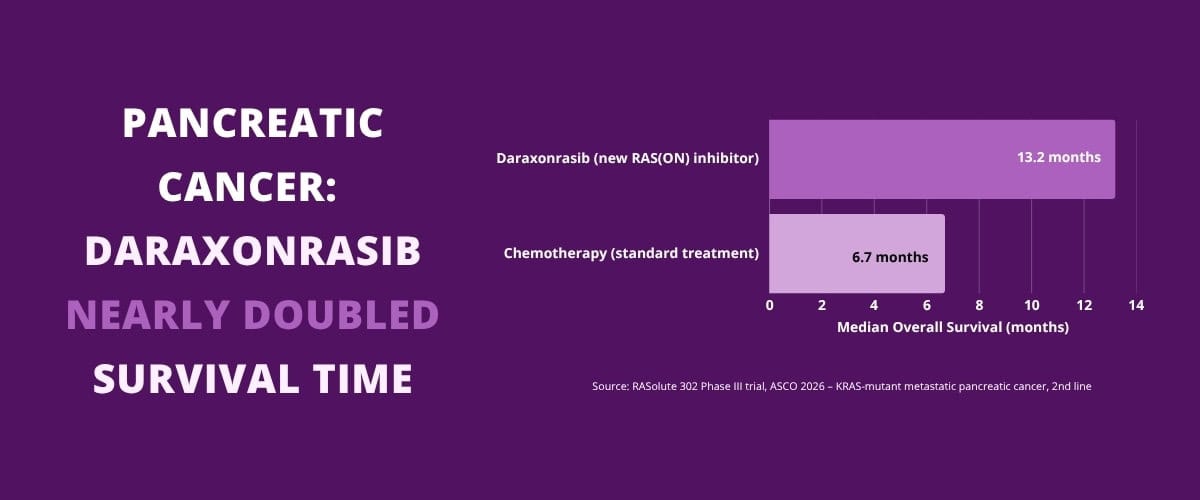
Trial results show that patients with advanced pancreatic cancer who received the new oral drug daraxonrasib lived for a median of 13.2 months, compared with 6.7 months on standard chemotherapy. That is a near doubling of overall survival, and it cuts the risk of death by 60%. For patients, or those with loved ones battling pancreatic cancer, this is very much welcomed good news.
Lung Cancer: Bispecific Antibodies Show Promise
Further good news in this difficult-to-treat group came from the HARMONi-6 trial, where an increasingly important class of drug called bispecific antibodies made significant improvement in responses as well as survival in late-stage lung cancer. The drug, ivonescimab, works by blocking two cancer-driving pathways – PD-1 and VEGF – simultaneously rather than just one, which is what current standard immunotherapy targets.
In the trial, patients with advanced squamous NSCLC who received ivonescimab alongside chemotherapy lived for a median of 27.9 months, compared with 23.7 months on the current standard immunotherapy plus chemotherapy. This is a meaningful step forward for a group of patients who, until now, had fewer options once their disease advanced.
Sarcoma: First Targeted Treatment for a Rare Type
Dedifferentiated liposarcoma is a rare and aggressive cancer of fatty tissue, and one that has had no effective targeted treatment so far. Patients who relapse after surgery have historically been left with chemotherapy options that control the disease for only a short time.
The SARC041 trial changed that, thanks to a finding that nearly all tumours of this type carry an amplified gene called CDK4, which drives its growth. Researchers reasoned that abemaciclib, a drug already used in breast cancer to block CDK4 and the related protein CDK6, could work here too. And it did.
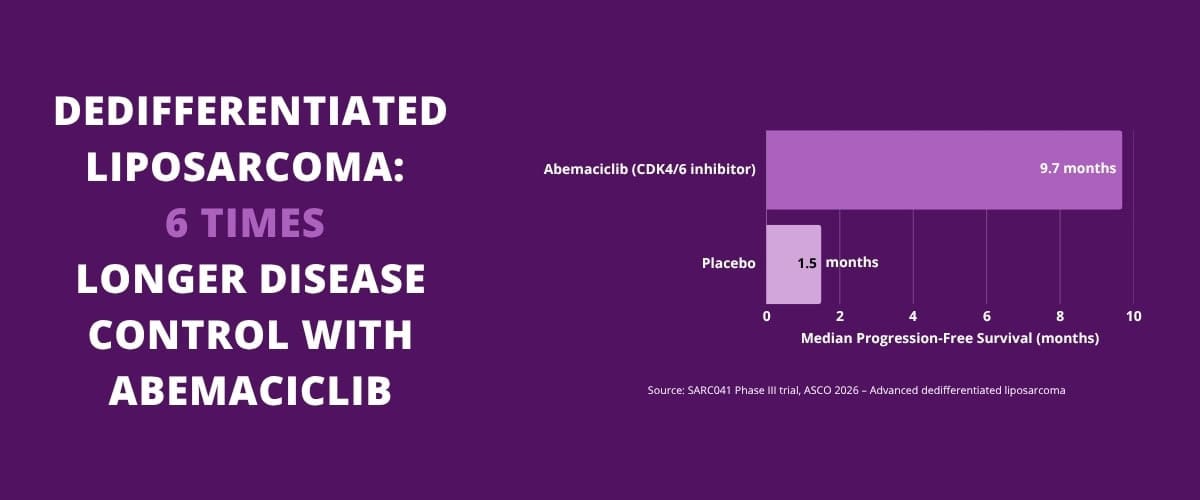
Patients treated with abemaciclib had their disease controlled for a median of 9.7 months, compared with just 1.5 months on placebo – roughly a six-fold improvement. This is the first time a targeted drug has shown clear benefit in this disease in a randomised trial. It is a reminder that even rare cancers, once their specific biology is well understood, can become treatable.
Prostate Cancer: Combining Hormone Therapy With Surgery Shows Improved Outcome
In treating prostate cancer, surgery – known as radical prostatectomy – is the first-line therapy for healthy patients with localised tumours. But for patients with high-risk, aggressive disease, more than half still relapse and go on to need further treatment.
The PROTEUS trial addressed relapse risk by adding hormone-blocking medication before and after surgery to prevent recurrence. Patients with high-risk localised or locally advanced prostate cancer received apalutamide together with standard hormone therapy for 6 months before and 6 months after their radical prostatectomy.
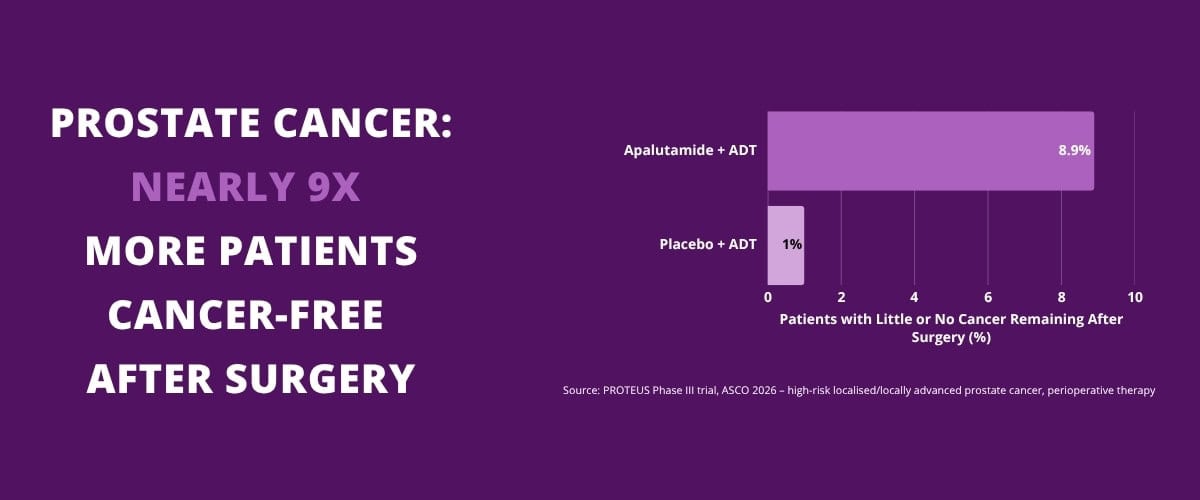
The results were striking. The rate of patients with little to no cancer remaining in the prostate after surgery rose from 1.0% to 8.9% – almost a nine-fold increase. Their risk of the cancer spreading or causing death fell by 20%. This is an encouraging shift towards treating aggressive prostate cancer earlier and more decisively to prevent recurrence.
Colorectal Cancer: More Treatment Options
In colorectal cancer, the BREAKWATER trial focused on a specific and historically difficult-to-treat group: patients whose tumours carry a mutation called BRAF V600E, found in roughly 1 in 10 metastatic colorectal cancers and associated with a poorer prognosis. Adding the targeted drugs encorafenib and cetuximab to standard chemotherapy nearly doubled the response rate compared with chemotherapy alone, and is set to become a new first-line standard for this group.
Breast Cancer: Smarter Chemotherapy, Less Surgery & New Options for Advanced Cancer
Back in 2018, I wrote about early results showing that some women with breast cancer do not need chemotherapy after surgery, based on genomic tests called Oncotype DX and Mammaprint. These tests analyse the genetic activity of a tumour to estimate how likely it is to come back. For the right patients, they help us confidently skip chemotherapy without compromising treatment outcomes.
This year’s OPTIMA trial extends this approach into a group of patients we previously assumed needed chemotherapy without question: those with clinically high-risk, ER-positive, HER2-negative early breast cancer, some with cancer in up to nine lymph nodes or larger tumours. A genomic test called Prosigna found that 68% of these patients had a low genomic risk of recurrence despite their high clinical risk.
For this group, skipping chemotherapy in favour of hormone therapy alone resulted in a five-year cancer-free survival rate of 93.6%, compared with 94.8% for those who received chemotherapy. The difference is small enough that the modest benefit of chemotherapy may not be worth its cost in side effects for many women.
We also have more data of this kind to show how we can de-escalate treatment if new reliable markers show that the cancer is already cured earlier. In these cases, there will be no necessity to continue with potentially toxic chemotherapy and/or immunotherapy.
Another de-escalation story involving breast cancer is about surgical decisions. Five-year data from the SENOMAC trial confirmed that women with early-stage breast cancer and only limited to the underarm lymph nodes do not need to have all of those lymph nodes removed. Overall survival was virtually identical – at 94.4% for those who skipped the full dissection versus 93.4% for those who had it. Avoiding the full lymph node removal brings a lifelong reduction in the risk of arm swelling and discomfort, or lymphedema, which can affect quality of life for decades after treatment.
For advanced breast cancer that has stopped responding to a CDK4/6 inhibitor – a common first-line treatment for hormone receptor-positive disease – the VIKTORIA-1 trial offered a new option: gedatolisib with fulvestrant extended progression-free survival by around 5.6 months over the current alternative.
Treatment Beyond the Tumour
A few other findings this year reminded me that cancer outcomes are shaped by more than the tumour alone.
GLP-1 medicines – the class used for weight management, such as semaglutide – were linked in one trial to a modest reduction in new breast cancers among overweight women without diabetes, and a notable 25% reduction in overall risk of death. This is an early but encouraging signal that metabolic health and cancer outcomes are more closely connected than we may have thought.
The CHALLENGE trial showed that exercise can be part of the treatment itself, not just good general advice. A structured, three-year exercise programme significantly lowered the risk of cancer recurrence in colon cancer survivors, compared with standard health education alone.
Artificial intelligence is also beginning to earn its place in oncology. When I watched demonstrations of new tools that can analyse pathology slides to help predict which patients may safely avoid chemotherapy, and flag patients at higher risk of cancer spreading to the brain before symptoms appear, I kept thinking of a future where treatment decisions could be made with more personalisation and precision than ever before.
What This Means for Cancer Patients and Families
For pancreatic cancer, lung cancer, and several other hard-to-treat conditions, we have more reasons to be hopeful than ever. The available options today are measurably better than a few years ago. And for many patients, the future of treatment may mean not more therapy, but maybe less therapy. More importantly, it is about the right therapy, to de-escalate cancer, prevent its recurrence and support patients in having a better quality of life after treatment.
It is still early days for several of these treatments, and not all of them are yet available or appropriate for every patient. If any of this is relevant to your situation or a loved one’s, I would encourage you to discuss it with your treating oncologist, who can advise on what applies to your specific diagnosis.
Dr Donald Poon